The 2014-2015 Flu Vaccine Ineffective What Should you Do?
Ivermectin + Mebendazole Cancer Succss Story
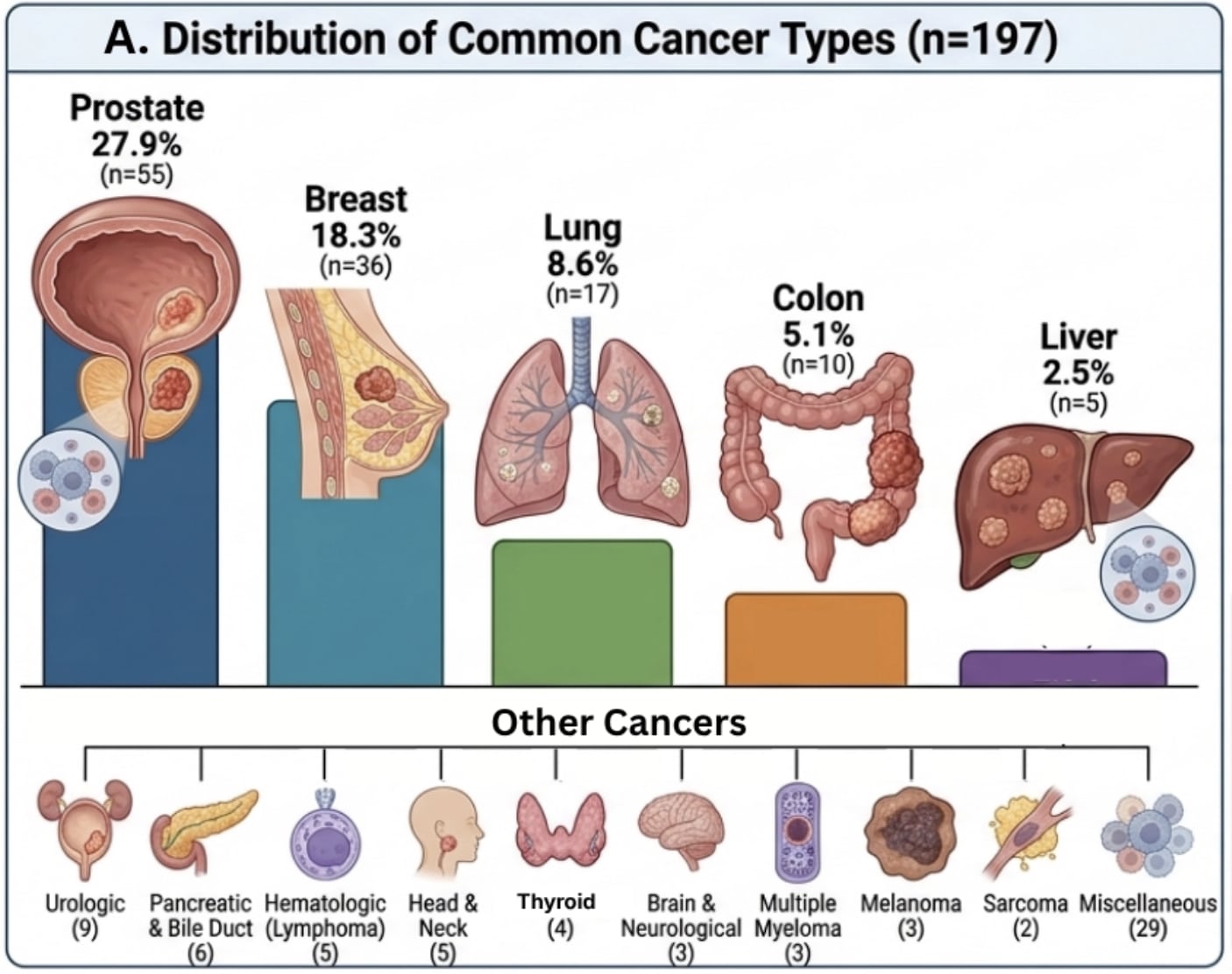
A new survey of 197 Cancer patients taking Ivermectin and Mebendazole for 6 months confirmed:
84.4% reported a clinical benefit
32.8% reported No evidence of disease
15.6% reported tumor regression
This confirms what we’ve seen in the 9000+ Cancer patients helped in the largest Ivermectin Cancer Project in the world!!
Dr. William Makis, MD, says, “I’ve often talked about a 75-80% clinical benefit that patients reported when they came to us, with some cancer patients getting tumor shrinkage, some getting stabilization of disease and some succeeding in preventing recurrence!” Now this study confirms an even higher Succes Rate of 84.4%
IVERMECTIN Cancer Revolution is here and it is going to be supported by more and more published studies!!