


Are You Getting Enough Vitamin D?
According to the International Journal of Health Sciences, “Vitamin D deficiency is a global vitamin deficiency. With all the medical advances of the century, vitamin D deficiency is still epidemic. Over a billion people worldwide are vitamin D deficient or insufficient. Yet no international health organization or governmental body has declared a health emergency to warn the public about the urgent need of achieving sufficient vitamin D blood levels.”
Multiple Studies are now showing that Low blood levels of Vitamin D are associated with an increased risk of getting COVID-19, suffering a more severe illness due to the infection and an increased risk of dying from it. A recent Retrospective Study, which measured Vitamin D levels in COVID-19 patients and the first Randomized Controlled Clinical Trial (RCT), which prescribed a high dose of Vitamin D to COVID-19 patients, have shown that Vitamin D deficiency appears to cause a significant risk when low and may provide significant benefit when supplemented in COVID-19 patients. Larger RCTs will be necessary to confirm these findings.
Vitamin D has hormone like activity. It regulates the functions of over 200 genes and is essential for growth, development and optimal immune function. Vitamin D deficiency is associated with susceptibility to acute respiratory tract infections, osteoporosis, obesity, diabetes, hypertension, depression, fibromyalgia, chronic fatigue syndrome and neuro-degenerative diseases including Multiple Sclerosis and Alzheimer’s disease. Vitamin D deficiency has even been associated with the development of cancers, especially breast, prostate, and colon cancers.
Unfortunately, finding an association of low Vitamin D does not prove that Vitamin D will prevent, treat or cure the disease. Nevertheless, the growing number of retrospective, prospective and Randomized Controlled Clinical Trials (RCTs) using Vitamin D is mounting. Taken together, these studies are beginning to build a compelling case for supplementing Vitamin D and highlighting the urgent need for more RCTs to confirm whether or not Vitamin D really works and what dose is required for it to be effective.

Recently, a group of Indonesian researchers, Raharusun et al, conducted a retrospective study on Vitamin D blood levels extracted from medical records of 780 Covid-19 patients from Indonesia, published on April 30, 2020.
Vitamin D deficiency levels were associated with dramatic increased incidence of death. The outcome differences were striking: “98.9% of Vitamin D deficient cases died, “while “only 4.1% of cases with normal Vitamin D levels died.”
Death Rate Declines Dramatically as Vitamin D Levels Rise
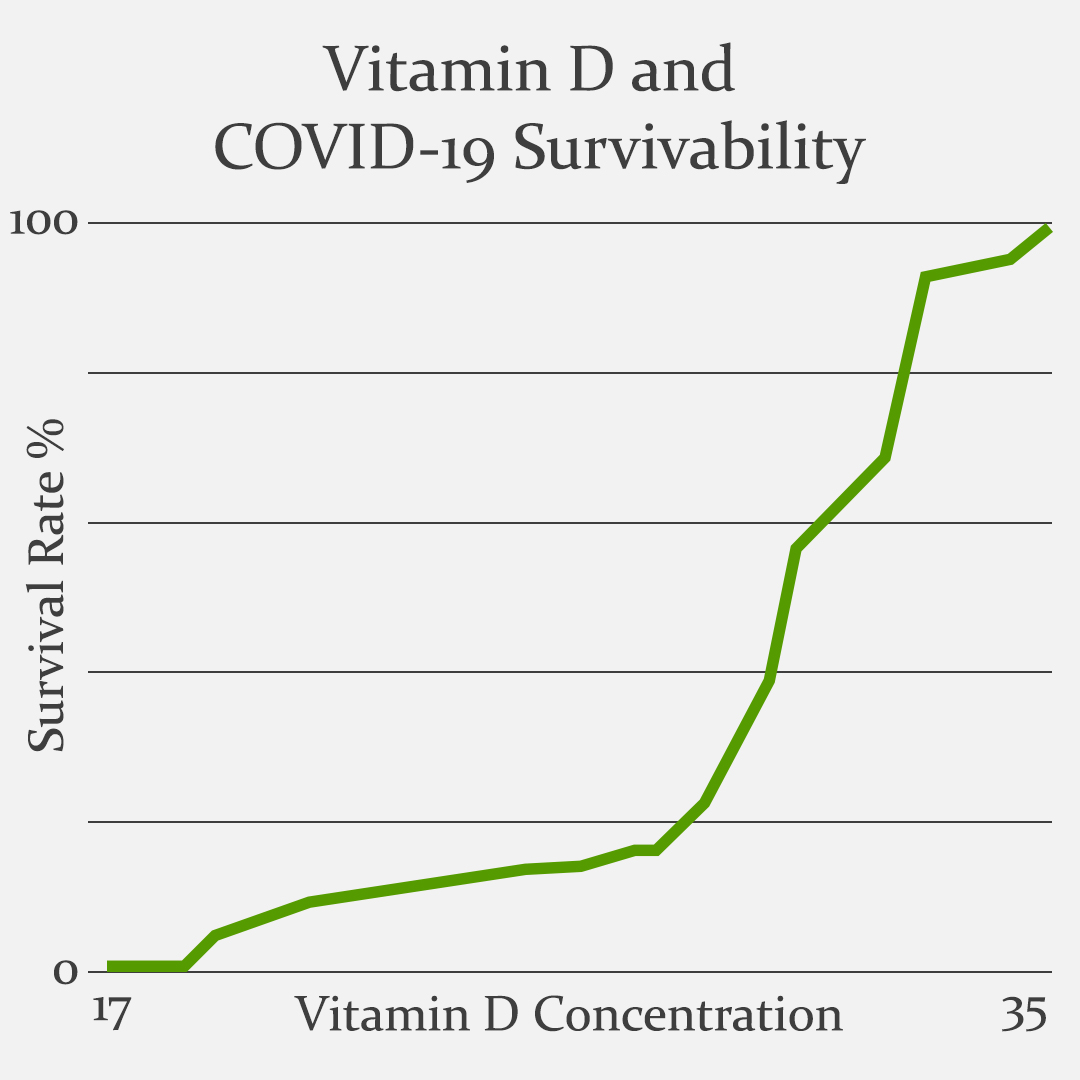
Data from the age-adjusted clinical study by the working group of Dr. Prabowo Raharusun.
Vitamin D level was the most striking correlation to survivability in this study, regardless of age, gender or number of comorbidities. If the Vitamin D blood level was 17ng/ml or lower on admission to the hospital, the patient died in 98.9% of the cases. If the Vitamin D blood level was above 30ng/ml only 4.1% of the patients died. I recommend that all my patients test and maintain a Vitamin D level of 50-70ng/ml year round.
Limitations of the Indonesia Vitamin D Study
This Retrospective Study was only an Observational Study rather than a Randomized Controlled Clinical Trial, which has not yet been peer reviewed. Vitamin D blood levels were measured but not administered as part of the treatment protocol. It is not known if the low Vitamin D levels associated with increasing risk of severity and death due to COVID-19 would be reduced by giving the patients Vitamin D, or what dose would be effective. A Randomized Clinical Trial is needed to determine whether or not administering Vitamin D would actually reduce COVID-19 cases and deaths.
The First Vitamin D COVID-19 Randomized Clinical Trial
The first Vitamin D COVID-19 Randomized Clinical Trial was conducted in Spain and published online in The Journal of Steroid Biochemistry and Molecular Biology on August, 29, 2020.
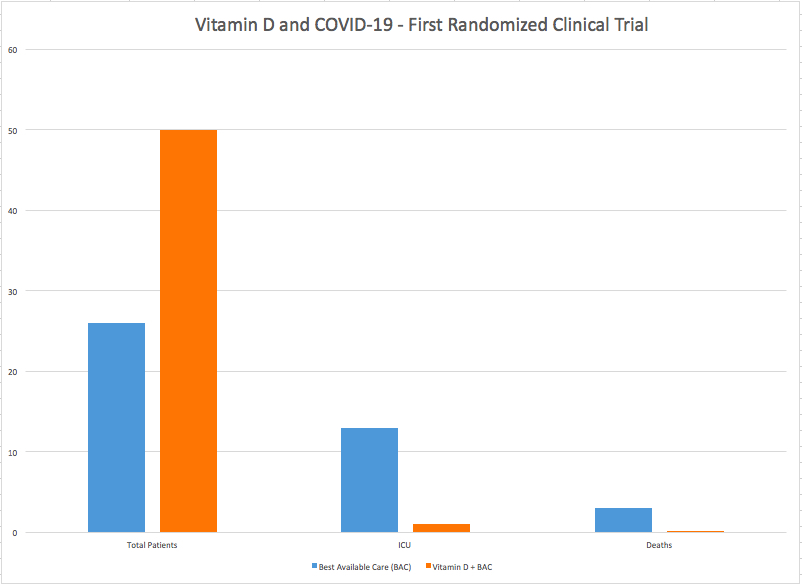
Of the 50 patients (Orange) treated with the current “Best Available Care” and Calcifediol (Vitamin D), only one (2%) required admission to the ICU and none died. Alternately, of the 26 patients (Blue) treated with “Best Available Care,” but without Calcifediol (Vitamin D), 13(50%) required admission to the ICU and 2 died (15%).
Highlights
- The vitamin D endocrine system has a variety of actions on cells and tissues involved in COVID-19 progression.
- Early calcifediol (25-hydroxy Vitamin D) treatment to hospitalized COVID-19 patients significantly reduced intensive care unit admissions.
- Calcifediol seems to be able to reduce the severity of the disease.
Researchers randomly allocated 76 Covid-19 patients into two groups. On the day of the hospital admission, the treatment group (50 patients) received “Best Available Care” (including HydroxyChloroquine + Azithromyocin) plus oral Calcifediol (Vitamin D). The control group (26 patients), received Best Available Care only and no Calcifediol (NoVitamin D). Oral Calcifediol was given at high doses of 532 mcg (20,280iu) on the first day and then at 266 mcg (10,640iu) on the third and seventh day, and then weekly until discharge or admission to the intensive care unit (ICU).
Of the 50 patients treated with Calcifediol (Vitamin D), only one (2%) required admission to the ICU, while of 26 patients treated without Calcifediol (Vitamin D), 13 (50%) required admission to the ICU.
Of the patients treated with Calcifediol (Vitamin D), none died, and all were discharged, without complications. The 13 patients not treated with Calcifediol, who were not admitted to the ICU, were discharged. Of the 13 patients not receiving Calcifediol (Vitamin D) who were admitted to the ICU, two died (15%) and the remaining 11 were discharged.
The Spain Vitamin D Study Conclusion: “Our pilot study demonstrated that administration of a high dose of Calcifediol, or 25-hydroxy Vitamin D, a main metabolite of vitamin D3 in the endocrine system, significantly reduced the need for ICU treatment of patients requiring hospitalization due to proven COVID-19. Calcifediol seems to be able to reduce severity of the disease, but larger trials with groups properly matched will be required to show a definitive answer.”
Results revealed that 13 out of 26 patients (50%) in the control group were admitted to ICU, and two died in the end. In the Calcifediol group, only one out of 50 (2%) required ICU admission, and none died. These results were statistically significant, equating to a 98% reduction in odds of ICU admission and 100% reduced risk of dying among ICU patients.
“Although this was a small trial, the ICU results are so dramatic that they are statistically highly significant,” according to a featured letter in The BMJ, a top-tier medical journal, in response to this clinical trial.
Limitations of Spain Vitamin D Study
As stated above, the key limitation of this study was that it was a very small study population. Another shortcoming was that all patients received Hydroxychloroquine and Azythromyocin. Therefore, it is not known how Calcifediol (Vitamin D) would work on its own. Calcifediol is 3.2 times more potent than natural Vitamin D3 supplements, therefore, it is not known if taking Vitamin D3 would be as effective or what dose of natural Vitamin D3 would be equivalent. Lastly, the researchers of this Study did not measure the Vitamin D3 levels of the patients before treatment for COVID-19, therefore, it is not known how Calcifediol (Vitamin D) affects the blood levels.
Benefit of the Spain Vitamin D Study
The Spain Vitamin D Randomized Clinical Trial provided the strongest evidence to date that Vitamin D3 therapy could work for COVID-19. These results support and confirm multiple prior studies that found that low Vitamin D3 levels in the blood is an independent risk factor for morbidity and mortality (disease and death) associated with COVID-19. This study found that oral Calcifediol (Vitamin D) reduced the risk of ICU admission by 98% compared to only 50% in the COVID-19 patient group that did NOT receive Calcifediol and ZERO deaths out of 50 patients in the Calcifdediol group vs 2 deaths out of 50 (4%) in the group that did not get Calcifediol.
Vitamin D Deficiency of Pandemic Proportions!
According to Healthline, it is estimated that about 1 billion people worldwide have low levels of Vitamin D in their blood. About 42% of the US population is Vitamin D deficient. However, this rate rises to 82% in black people and 70% in Hispanics, because the increased amount of melanin in darker skin blocks the absorption of UV-B sunlight, which is required to make Vitamin D in the skin.
According to research updated on September 21, 2020, in Medscape Endocrinology online, Vitamin D insufficiency is highest among people who are elderly, institutionalized, or hospitalized. In the United States, 60% of nursing home residents and 57% of hospitalized patients were found to be Vitamin D deficient.
The major circulating form of vitamin D is 25-hydroxy Vitamin D [25(OH)D]; thus, the total serum 25(OH)D level is currently considered the best indicator of vitamin D supply to the body from cutaneous synthesis and nutritional intake.
The reference range of the total 25(OH)D level is 25-80 ng/mL. Vitamin D deficiency is defined by most experts as a serum Hydroxy Vitamin D [25(OH)D] level of less than 20 ng/mL (50 nmol/L). The average adult Vitamin D blood level across the US is 20-26 ng/mL.
LABORATORY Blood Levels of Vitamin D (25-Hydroxy Vitamin D)
- Deficiency: Less than 20 ng/ml (50 nmol/L)
- Insufficiency: 21-29 ng/mL (52-72 nmol/L)
- Sufficiency: 30 ng/mL (75 nmol/L) or above
- Optimal: 50-70ng/mL(125-175nmol/L)
- Excessive: greater than 100ng/mL (250nmol/L)
France, Spain and Italy have the highest numbers of COVID-19 cases in Europe. In France the mean adult Vitamin D level is 17.2. In Spain it is a very low 10.4 ng/mL. In Italy it is only slightly higher at 11.2 ng/mL. Italy has a high correlation of Vitamin D deficiency and severity of COVID-19 cases.
Low Vitamin D levels are found most frequently in northern latitudes and are associated with low levels of sunlight, older age, darker skin and a diet deficient in Vitamin D rich foods.
Researchers found that people in the Nordic countries have higher levels of Vitamin D because they tend to seek more outdoor sunshine, consume more Vitamin D supplements and eat more fish high in Vitamin D, which may account for their higher blood levels. The mean level of Vitamin D in Nordic countries is 18.0 ng/mL.
Vitamin D insufficiency is obviously not restricted only to the elderly and hospitalized population. Several studies have found a high prevalence of Vitamin D deficiency among healthy, young adults as well. Nearly two thirds of healthy, young adults in Boston become vitamin D insufficient at the end of each winter.
An analysis of data of almost 3000 US children and adolescents (age, 6-18 y) from the National Health and Nutrition Examination Survey (NHANES) 2003-2006 indicated that, based on current Institute of Medicine Committee guidelines, about 10.3% of this population (an estimated 5.5 million) had inadequate vitamin D (25(OH)D) blood levels (< 16 ng/mL), and 4.6% (an estimated 2.5 million) had levels placing them at risk of frank deficiency (< 12 ng/mL). Adolescents (age, 14-18 y) and obese children had the highest risk of 25(OH)D deficiency and inadequacy, and these risks were also higher among girls than boys (of any age and body mass index) and among nonwhite children.
How Does Vitamin D Work?
Vitamin D works by enhancing calcium metabolism, cardiovascular function and immunity. The active form of Vitamin D is essential to the body’s innate and adaptive immune systems, where it produces specialized Anti-Microbial Peptides (AMPs) known as Cathelicidin and Defensins, which reduce the survival and replication of viruses.
Vitamin D also assists in regulating inflammatory cytokines. Vitamin D initially enhances inflammatory cytokines to kill viruses and other microbes and then suppresses inflammation to prevent a cytokine storm when the infection is under control. Vitamin D is widely recognized for its ability to balance the immune response.
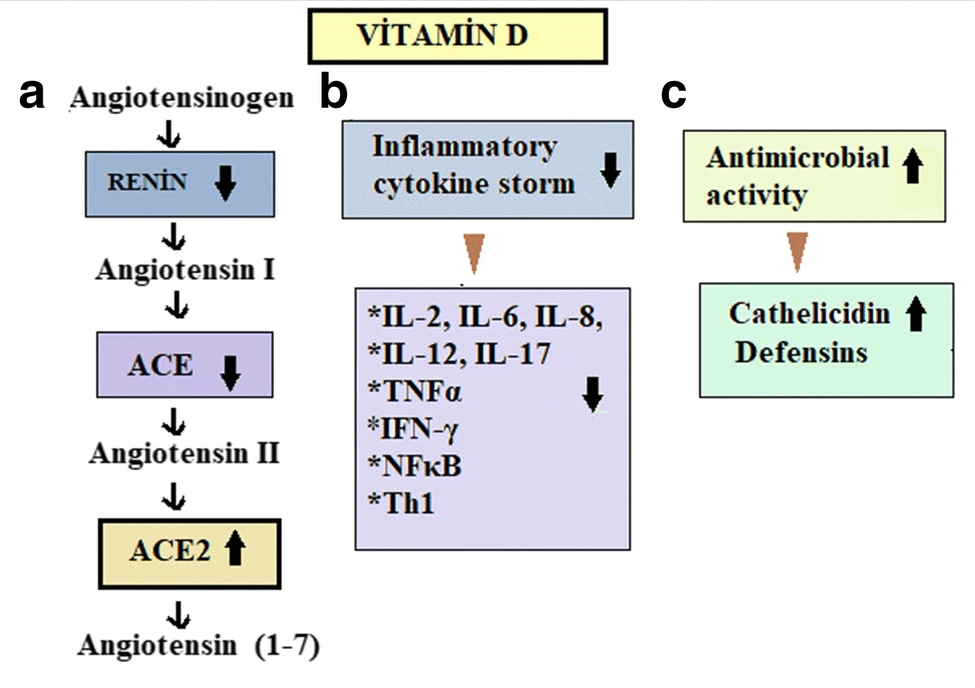
a Vitamin D might prevent the development of ARDS, hypertension, and cardiovascular system disorders by reducing the level of renin, ACE, and angiotensin II and increasing the level of ACE2. b It can prevent the development of oxidative stress and organ damage by reducing inflammatory cytokines in many tissues. c Vitamin D may enhance antimicrobial activity by increasing defensins and cathelicidins peptides level. This could be effective against the COVID-19 infection. Image courtesy of Hatice Aygun. “Vitamin D can prevent COVID-19 infection-induced multiple organ damage.” Source: Archives of Pharmacology, 17 May 2020; Vitamin D Can Prevent COVID-19 Infection-Induced Multiple Organ Damage.25
Key immune cells, including dendritic cells, monocytes, macrophages, as well as B cells and T cells, have been shown to possess vitamin D receptors (VDR) capable of converting 25-hydroxy Vitamin D (25OHD) into the active form of Vitamin D [1,25-(OH)2 D]. This allows these immune cells to make active Vitamin D at the site of infections and inflammation. When active Vitamin D binds to the VDR it allows the Vitamin D to move into the cell nucleus where it modifies the expression of hundreds of genes to fight infectious organisms and control inflammation.
The Coronavirus, SARS-CoV-2, is known to specifically bind to ACE2 receptors in humans, in order to get inside the cells of the lungs and other tissues, where it replicates and multiplies, leading to severe inflammation, pneumonia, tissue damage, and organ failure. Vitamin D is known to block Renin, ACE and Angiotensinogen II and increase ACE2, which reduces excessive inflammation and the risk of Acute Respiratory Distress Syndrome (ARDS), myocarditis, or cardiac injury. Vitamin D treatment may decrease the risk of incidence of the COVID-19 infection by increasing the ACE2 level, which may significantly decrease the mortality and severity of COVID-19.
Vitamin D deficiency has been linked to increased susceptibility to viral infections and multiple organ failure. More and more Vitamin D studies are finding that Vitamin D deficiency is directly associated with susceptibility to COVID-19 morbidity and mortality, and that Vitamin D supplementation could support the immune defenses that help it decrease the risk and severity of COVID-19. Additional Randomized Clinical Trials are needed to confirm the numerous mechanistic and retrospective studies that indicate its essential importance.
How to Get More Vitamin D
Vitamin D can be synthesized by the body in the skin when exposed to Ultraviolet-B (UV-B) in sunlight. We also get Vitamin D from fatty fish like tuna, mackerel, and salmon, as well as beef liver, cheese and egg yolks. If you have lighter skin and access to strong sun all year, then 15-20 min of sun exposure over 40% of your body daily, may be enough to fulfill your vitamin D requirements. However, if you live far north or south of the equator then your vitamin D levels may be deficient due to decreased sunshine and the season of the year. The levels may go down during the winter months, due to a lack of sufficient sunlight. For these reasons you should get a blood test to measure the amount of Vitamin D actually in your blood stream. I recommend getting at least 20 minutes of sunshine over 40% of your body at least oncer per week and taking enough Vitamin D3 daily (typically 5000-6000iu daily for adults) to maintain your blood level of 25-HydroxyD at 50-70ng/mL year round.
How Much Vitamin D is Enough?
There is currently no scientific consensus about the optimal dose of Vitamin D supplementation for COVID-19. Currently, The Institute of Medicine has placed the recommended dietary allowance, or RDA, for vitamin D at 600 international units (IU) per day for young adults and 800 IU per day for adults older than 70 years. But this recommendation was issued in context with bone health. Based on observational studies, concentrations of at least 40-50 ng/mL are desired. Another study reported that 38 ng/mL was suitable for reducing the risk of community acquired pneumonia.
Source: Joseph Mercola, DO, Vitamin D in the Prevention of COVID-19.26
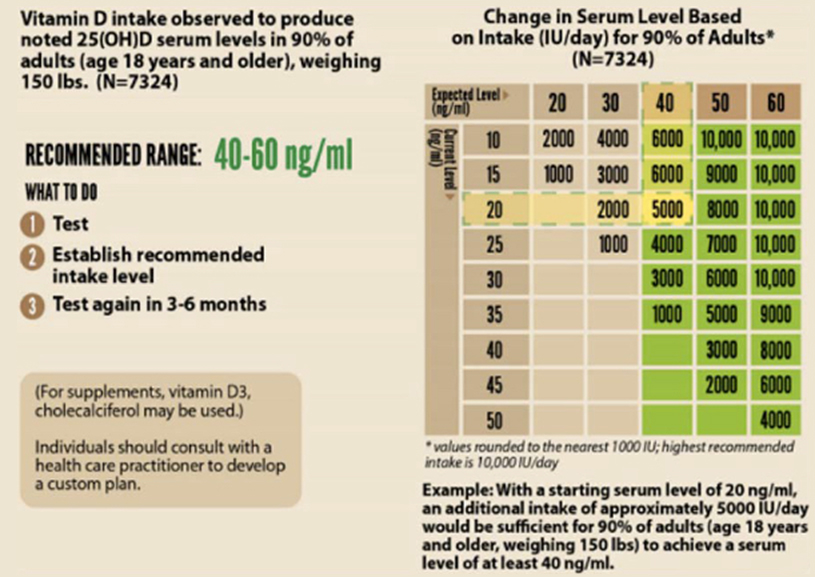
In order to achieve the above concentration range, dose of 2000-5000 IU/day of Vit D3 could be taken. A study reported that in order to increase your Vitamin D3 level from 20ng/mL up to 39mg/mL you will need to take 4000 IU/day. If you want to get it up 64ng/ml you will need to supplement 10,000 IU/day for 8 weeks.
The U.S. Institute of Medicine noted that for daily doses of < 10,000 IU/day no adverse effects have been reported for Vit D supplementation. (Vitamin D Levels and COVID-19 Susceptibility: Is there any Correlation?
Twenty minutes of sensible non-burning sunbathing by pale-skinned-humans, can produce 20,000 IU (Holick, M. (2011). ‘Vitamin D: a d-lightful solution for health’, Journal of investigative medicine : the official publication of the American Federation for Clinical Research, 59(6), p.872–880. DOI: 10.2310/JIM.0b013e318214ea2d)
Ideally one should test their vitamin D blood level as this will help to understand the appropriate starting dose. If the level is about 20 ng/mL it takes about 85 days to reach 60ng/mL with a daily dose of 4,000iu/day, but only 35 days if you take a daily dose of 10,000 IU/day.
If one is challenged with an acute immune challenge, it may be wise to take a very large initial dose. A randomized controlled trial (RCT) published in 2015 showed that after a single dose of 250,000 IU of vitamin D3 given to healthy volunteers between the ages of 18 and 65 years with baseline serum levels of <17 ng/ml, serum 25(OH)D concentrations increased to an average of 41 ng/ml after five days with no adverse effects.
After taking the single mega-dose of Vitamin D3, I recommend taking a daily dose of 5,000iu (international units) once daily, to maintain optimal Vitamin D levels and immune benefits.
Can You Get Too Much of a Good Thing?
According to the 2015 Mayo Clinic Proceedings, Vitamin D Toxicity and hypercalcemia are exceedingly rare. “The evidence is clear that Vitamin D toxicity is one of the rarest medical conditions and is typically due to intentional or inadvertent intake of extremely high doses of vitamin D, usually in the range of >50,000 – 100,000 IU/day for months to years.”
I recommend that everyone get a blood test to determine their Vitamin D level (Vitamin D, 25-Hydroxy; AKA: 25-Hydroxycalciferol, 25-OH-D, Colecalciferol Metabolite, or Vitamin D3 Metabolite); Most Americans who do not take a Vitamin D3 Supplement tend to have a Vitamin D3 blood level of 22-26 ng/ml. Ideally it should be 50-70ng/mL. I recommend taking 5000iu of Vitamin D3 daily year round to keep your blood levels in the optimum range. You may need to take more if you are over age 70 (because you will absorb less), obese (because you tend to store more in excess fat tissue), or have darkly pigmented skin (because melanin blocks UV-B sun rays from making natural Vitamin D in you skin.
Summary
A Review of the Vitamin D research by COVID.US.ORG states, “There is now enough evidence for treatment with Calcifediol (Vitamin D3), also known as 25(OH)D, to be STANDARD CARE for hospitalized patients with COVID-19. There is enough evidence for Vitamin D supplementation to be recommended to everyone at risk of COVID-19, especially those at high risk. And since the elderly often have difficulty absorbing Vitamin D, they should receive a higher dosage.”
Vitamin D is an essential nutrient cofactor for optimal immune function. It is not a drug and does not prevent, treat or cure COVID-19, but it supports the body’s inherent, God-given Immune System operations to achieve its optimal function to prevent viruses from multiplying inside our bodies and the immune system can then perform its function optimally and stop the virus from causing serious harm, or reduce serious morbidity and mortality.
Vitamin D References
- Alipio, Mark. “Vitamin D Supplementation Could Possibly Improve Clinical Outcomes of Patients Infected with Coronavirus-2019 (COVID-19).” SSRN 3571484 (9 April 2020). Study Link | PDF Link
- Lau, Frank H., et al. “Vitamin D insufficiency is prevalent in severe COVID-19.” medRxiv (28 April 2020). Study Link | PDF Link
- Daneshkhah, Ali, et al. “The Possible Role of Vitamin D in Suppressing Cytokine Storm and Associated Mortality in COVID-19 Patients.” medRxiv (2020). Study Link | PDF Link
- Davies, Gareth, Attila R. Garami, and Joanna C. Byers. “Evidence Supports a Causal Model for Vitamin D in COVID-19 Outcomes.” medRxiv (2020). Study Link | PDF Link
- De Smet, Dieter, et al. “Vitamin D deficiency as risk factor for severe COVID-19: a convergence of two pandemics.” medRxiv (2020). Study Link | PDF Link
- Raharusun, Prabowo, et al. “Patterns of COVID-19 Mortality and Vitamin D: An Indonesian Study.” (2020). PDF file | PDF Link
- Ilie, Petre Cristian, Simina Stefanescu, and Lee Smith. “The role of vitamin D in the prevention of coronavirus disease 2019 infection and mortality.” Aging Clinical and Experimental Research (2020): 1. Study Link | PDF Link
- D’Avolio, Antonio, et al. “25-hydroxyvitamin D concentrations are lower in patients with positive PCR for SARS-CoV-2.” Nutrients 12.5 (2020): 1359. Study Link | PDF Link
- Laird, E., et al. “Vitamin D and Inflammation: Potential Implications for Severity of Covid-19.” Ir Med J; Vol 113; No. 5; P81: 2020. PDF file | PDF Link
- Faul, J.L., et al. “Vitamin D Deficiency and ARDS after SARS-CoV-2 Infection.” Ir Med J; Vol 113; No. 5; P84: 2020. PDF file | PDF Link
- Meltzer, David O., et al. “Association of Vitamin D Deficiency and Treatment with COVID-19 Incidence.” medRxiv (2020). Study Link | PDF Link
- Li, Yajia, et al. “Sunlight and vitamin D in the prevention of coronavirus disease (COVID-19) infection and mortality in the United States.” (2020). PDF file | PDF Link
- Pugach, Isaac Z. and Pugach, Sofya “Strong Correlation Between Prevalence of Severe Vitamin D Deficiency and Population Mortality Rate from COVID-19 in Europe.” medRxiv (2020). Study Link | PDF Link
- Merzon, Eugene, et al. “Low plasma 25(OH) vitamin D3 level is associated with increased risk of COVID-19 infection: an Israeli population-based study.” medRxiv (2020). — Low vitamin D increased risk (adjusted OR) of infection with Covid-19 by 45% and of hospitalization for Covid by 95%. Study Link | PDF Link
- Panagiotou, Grigorios et al., “Low serum 25-hydroxyvitamin D (25[OH]D) levels in patients hospitalised with COVID-19 are associated with greater disease severity: results of a local audit of practice.” medRxiv (2020). Conclusion: “we found that patients requiring ITU admission [in the ICU] were more frequently vitamin D deficient than those managed on medical wards [on the floor], despite being significantly younger.” PDF file Link | PDF Link
- Chang, Timothy S., et al. “Prior diagnoses and medications as risk factors for COVID-19 in a Los Angeles Health System.” medRxiv (2020). Study Link | PDF Link
~ Risk factors included vitamin D deficiency, which increased risk of COVID-19 diagnosis by 80% (OR 1.8 [1.4-2.2], p=5.7 x 10-6). - Maghbooli, Zhila, et al. “Vitamin D Sufficiency Reduced Risk for Morbidity and Mortality in COVID-19 Patients.” Available at SSRN 3616008 (2020). Study Link | PDF Link
~ Vitamin D sufficiency reduced clinical severity and inpatient mortality. - Panarese and Shahini, “Letter: Covid-19 and Vitamin D” Alimentary Pharmacology and Therapeutics, April 12, 2020. Link to Letter | PDF Link
~ Covid-19 mortality increases with increasing latitude (by nation), and vitamin D blood levels decrease with increasing latitude. The authors propose that low levels of vitamin D increase Covid-19 mortality. - Carpagnano, Giovanna Elisiana, et al. “Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19.” Journal of Endocrinological Investigation (2020): 1-7. Study Link | PDF Link
~ “A survival analysis highlighted that, after 10 days of hospitalization, severe vitamin D deficiency patients had a 50% mortality probability, while those with vitamin D = 10 ng/mL had a 5% mortality risk (p = 0.019).” - Mardani, R., et al. “Association of vitamin D with the modulation of the disease severity in COVID-19.” Virus Research (2020): 198148. Study Link | PDF Link
- Castillo, Marta Entrenas, et al. “Effect of Calcifediol Treatment and best Available Therapy versus best Available Therapy on Intensive Care Unit Admission and Mortality Among Patients Hospitalized for COVID-19: A Pilot Randomized Clinical study.” The Journal of Steroid Biochemistry and Molecular Biology (2020): 105751. Study Link | PDF Link
- Radujkovic, et al. “Vitamin D Deficiency and Outcome of COVID-19 Patients.” Nutrients 2020, 12(9), 2757; Study Link | PDF Link
— “The present study demonstrates an association between VitD deficiency and severity of COVID-19.
VitD-deficient patients had a higher hospitalization rate and required more (intensive) oxygen therapy
and IMV. In our patients, when adjusted for age, gender, and comorbidities, VitD deficiency was
associated with a 6-fold higher hazard of severe course of disease and a ~15-fold higher risk of death.” - Karan Razdan, Kuldeep Singh, Dilpreet Singh. Vitamin D Levels and COVID-19 Susceptibility: Is there any Correlation? Available online 2 June 2020. PDF Link
- Hanff TC, Harhay MO, Brown TS, Cohen JB, Mohareb AM (2020) Is there an association between COVID-19 mortality and the renin- angio-tensin system–a call for epidemiologic investigations. Clin Infect Dis. article link
- Hatice Aygun. Vitamin D can prevent COVID-19 infection-induced multiple organ damage. Archives of Pharmacology. Received: 6 April 2020 / Accepted: 17 May 2020. Faculty of Medicine, Tokat Gaziosmanpasa University, 60030 Tokat, Turkey. Article Link.
- Joseph Mercola, DO, Vitamin D in the Prevention of COVID-19, June 23, 2020. PDF Link